Active Labor: A Medical Label That Doesn’t Work for Us
As a birth doula trainer I'm seeing a disturbing trend: Workshop participants coming to their training workshops carrying trauma from having poor, disengaged and highly dissatisfying experiences with their own doulas. While participants arriving with birth trauma is nothing new, the cause being from poor experiences with their own doulas is new and alarming.
In my work as a hospital-based doula, I've had to support clients whose privately hired doulas neglected their clients' needs for emotional, physical and advocay support when they refused to physically come until 'active labor' or a specific cervical dilation.
These observations show the following problems:
- Doulas misuse and misunderstand what active labor is, a medical term used by medical care givers that marks the acceleration of cervical dilation, which leads to doulas showing up far too late in labor to provide adequate support.
- Clients experience dissatisfaction, abandonment and even emotional trauma from a lack of support.
- Educators, trainers and training materials are inaccurate at teaching the physiological phases of labor.
When I look historically why we're seing this issue now, it could have originated when ACOG redefined active labor in 2014. While “6 is the new 4” is an accurate and appropriate medical redefinition for the expected acceleration of cervical dilation, "6 is the new 4" should never have changed when doulas show up for in-person support. Nor should it have changed how educators or trainers teach the physiologic phases of labor, which, of course, did not change with the medical redefinition of active labor.
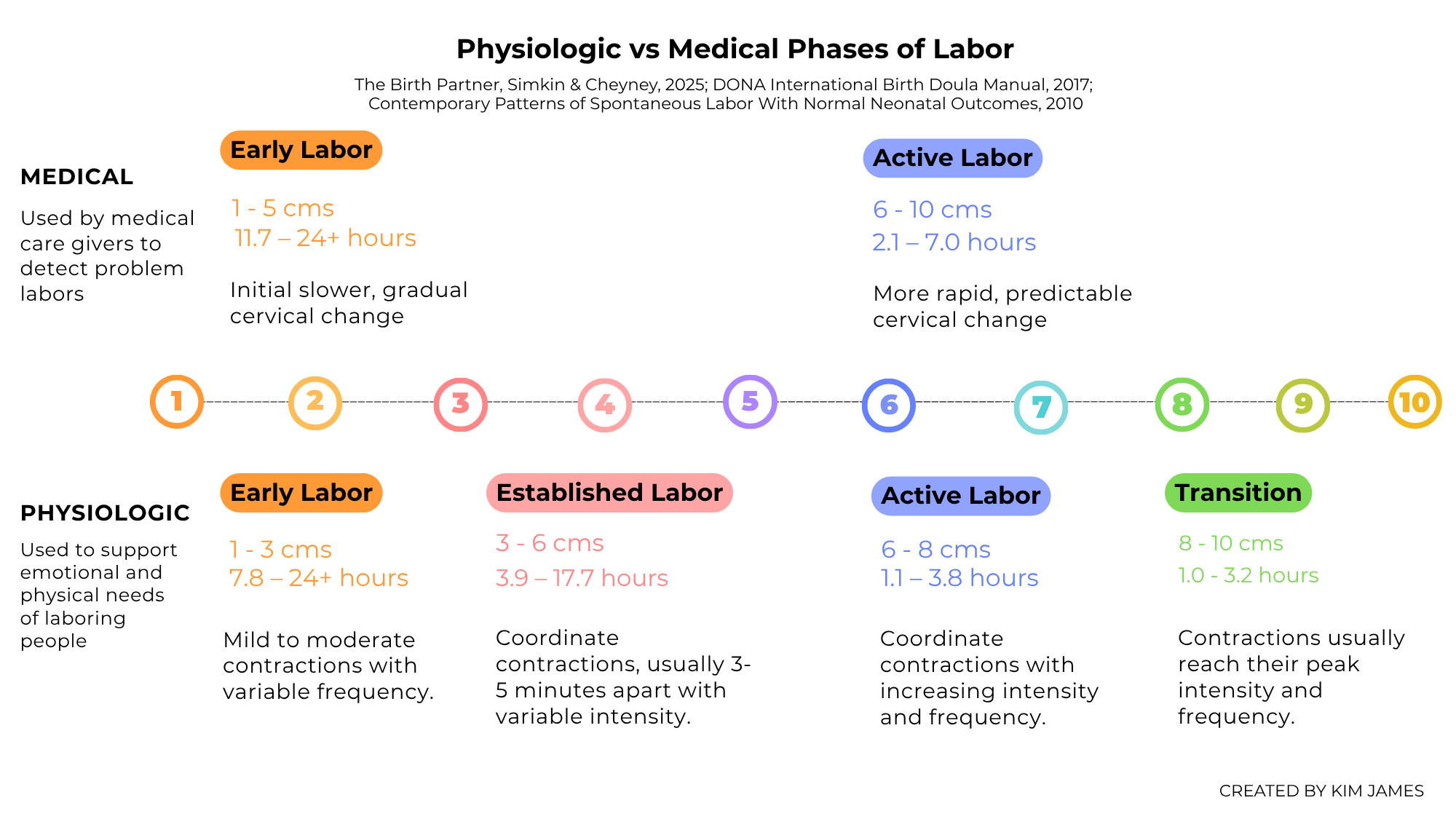
Medically, active labor is an important obstetrical benchmark for detecting slow labors that require attention and arrested labors that require action. Using partograms based on the Zhang labor curves where 6 cms is the threshold for active labor, obstetrical care providers can better identify truly problem labors.
Before the redefinition of active labor in 2014, the medical phases and stages of labor more closely lined up with the physiologic phases labor. See this Stages of Labor graphic from Childbirth Graphics that was published and used in childbirth education classes and doula workshops before 2014:
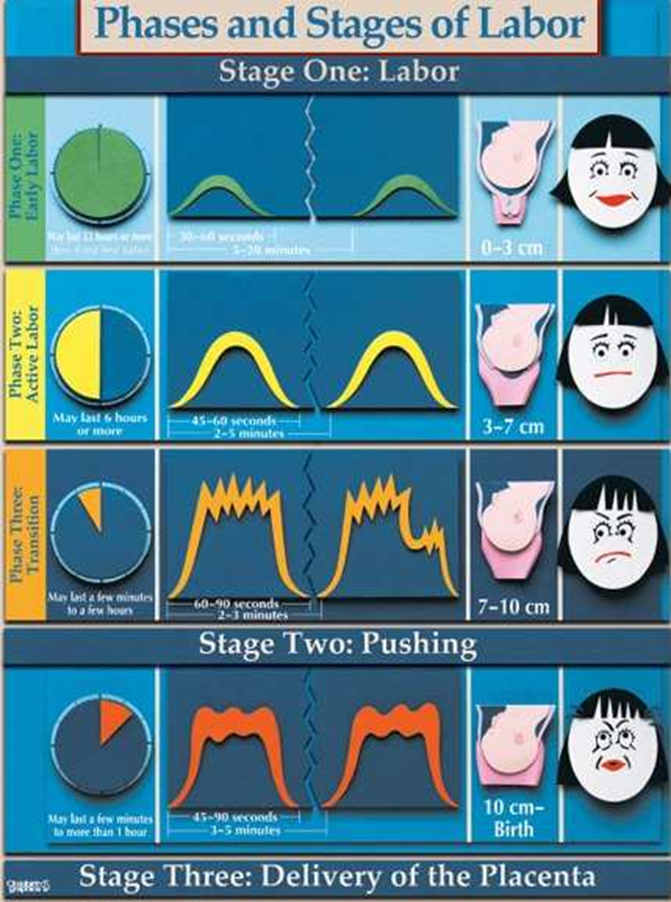
Once active labor was redefined to 6 cms rather than 4 cms, the medical phases and stages of labor took a sharp turn away from the physiologic phases and stages.
Unfortunately, our teaching aids and the way we teach the physiologic phases of labor changed along with the medical definition of active labor. This doesn’t work. When we look at this updated Stages of Labor graphic from Childbirth Graphics, it now shows 0-6 cms having the same physical and emotional characteristics as the previous 0-3 cms early labor phase. Of course, this isn’t true.
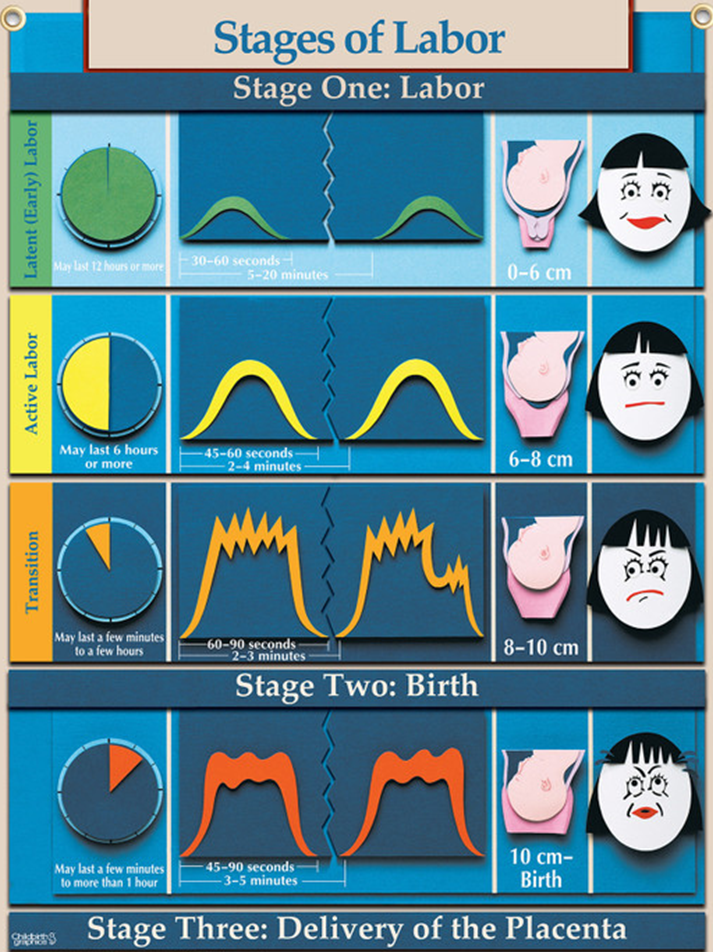
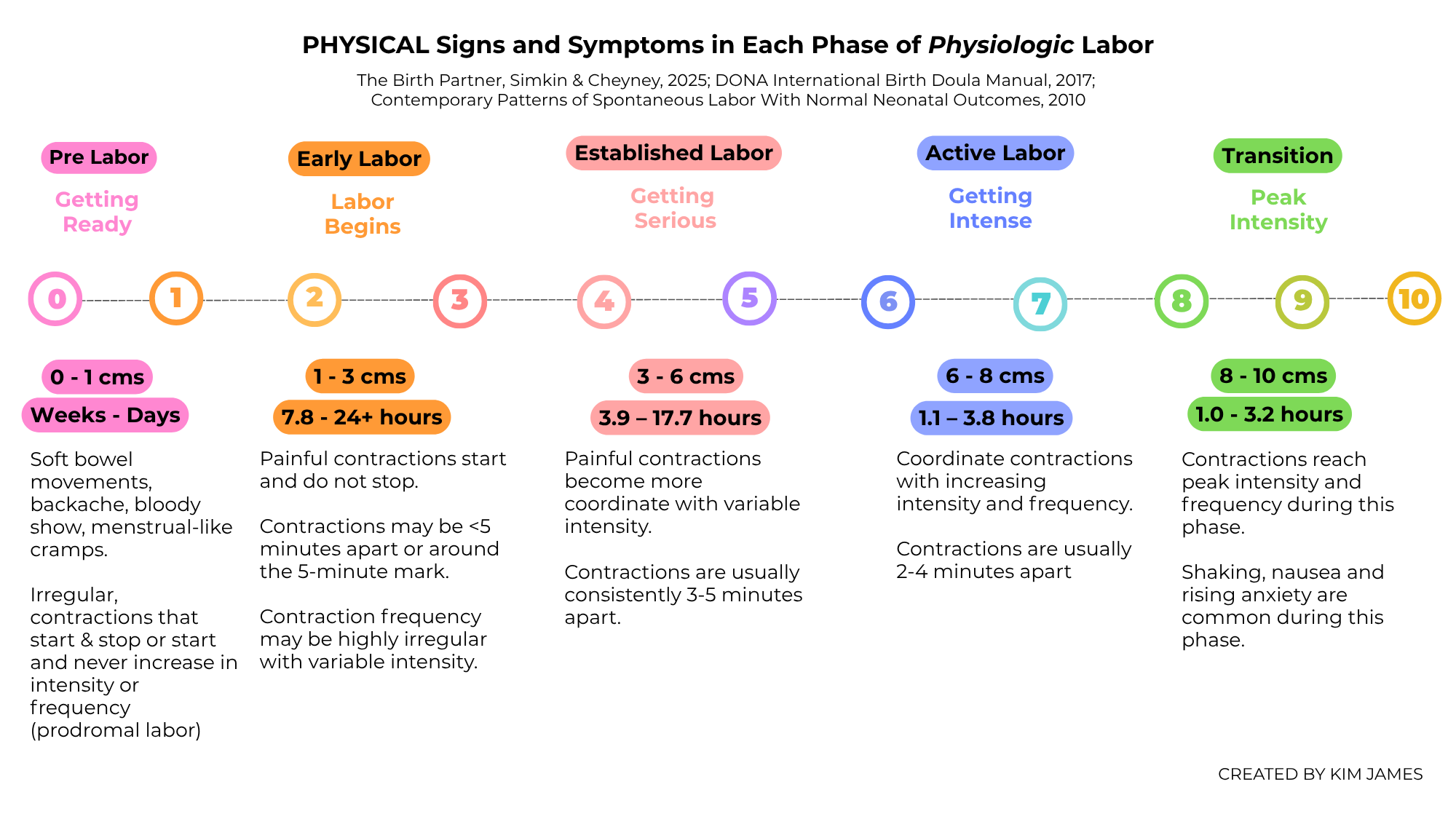
This graphic, because it confuses the medical early labor phase with the physiologic early labor phase, sets up doulas, parents, educators and trainers with unrealistic, false expectations for what the physiologic early Labor phase really is: A phase of labor with significant periods of increasing physical intensity and changing emotional needs.
“6 is the new 4” changed the definition of active labor for medical care givers, who use that definition as a very specific way to guide medical decisions. "6 is the new 4" DOES NOT WORK FOR US! Physiologic labor did not change when the medical redefinition of active labor did.
Let’s look at a solution: Changing the language doulas and educators use when we describe the physiologic phases of labor so that we are not mistakenly using medical terms and medical definitions.
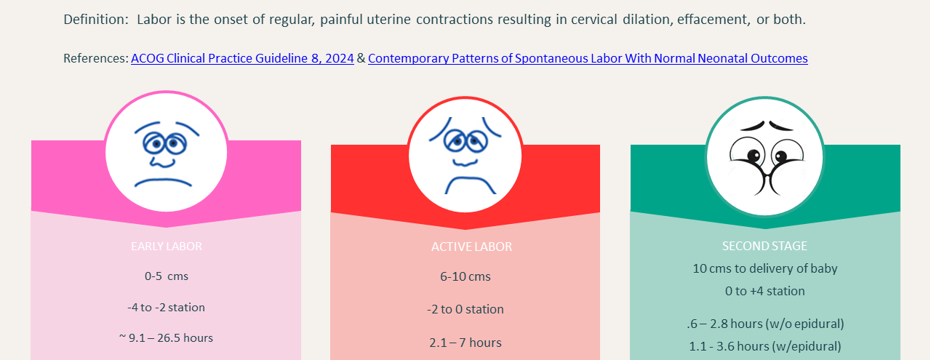
First, here is how ACOG defines the medical onset, phases and stages of labor:
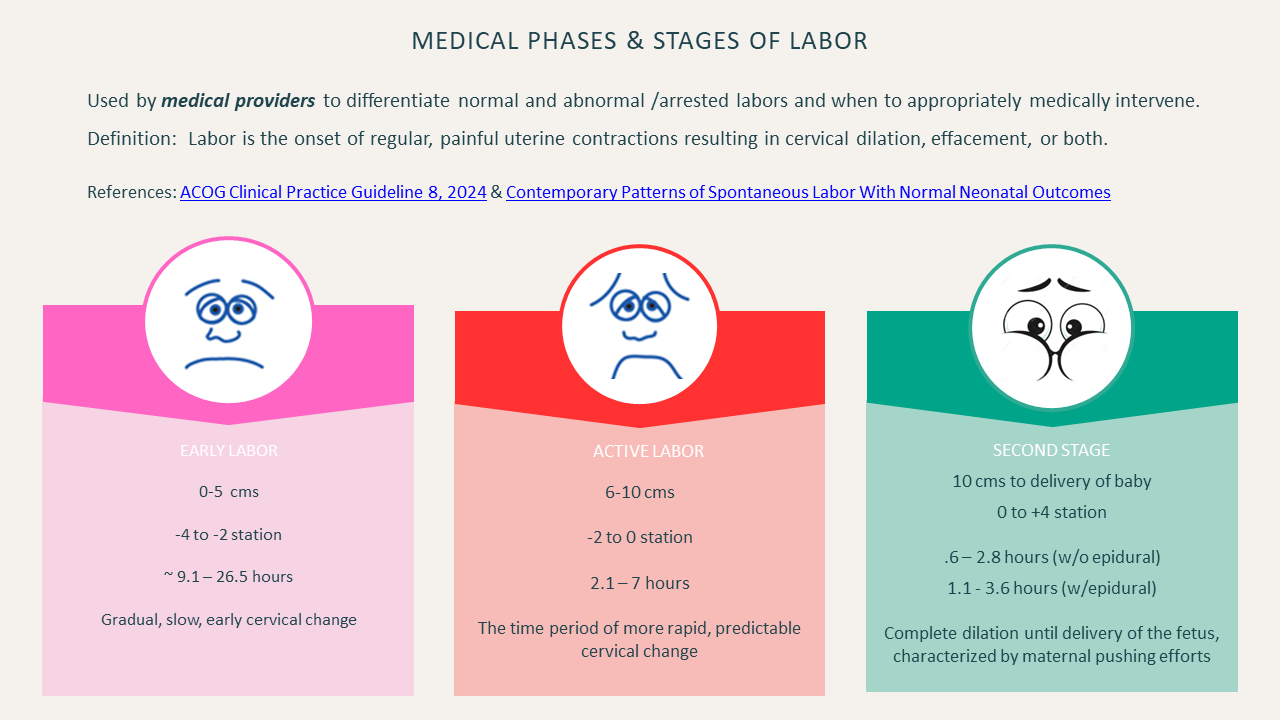
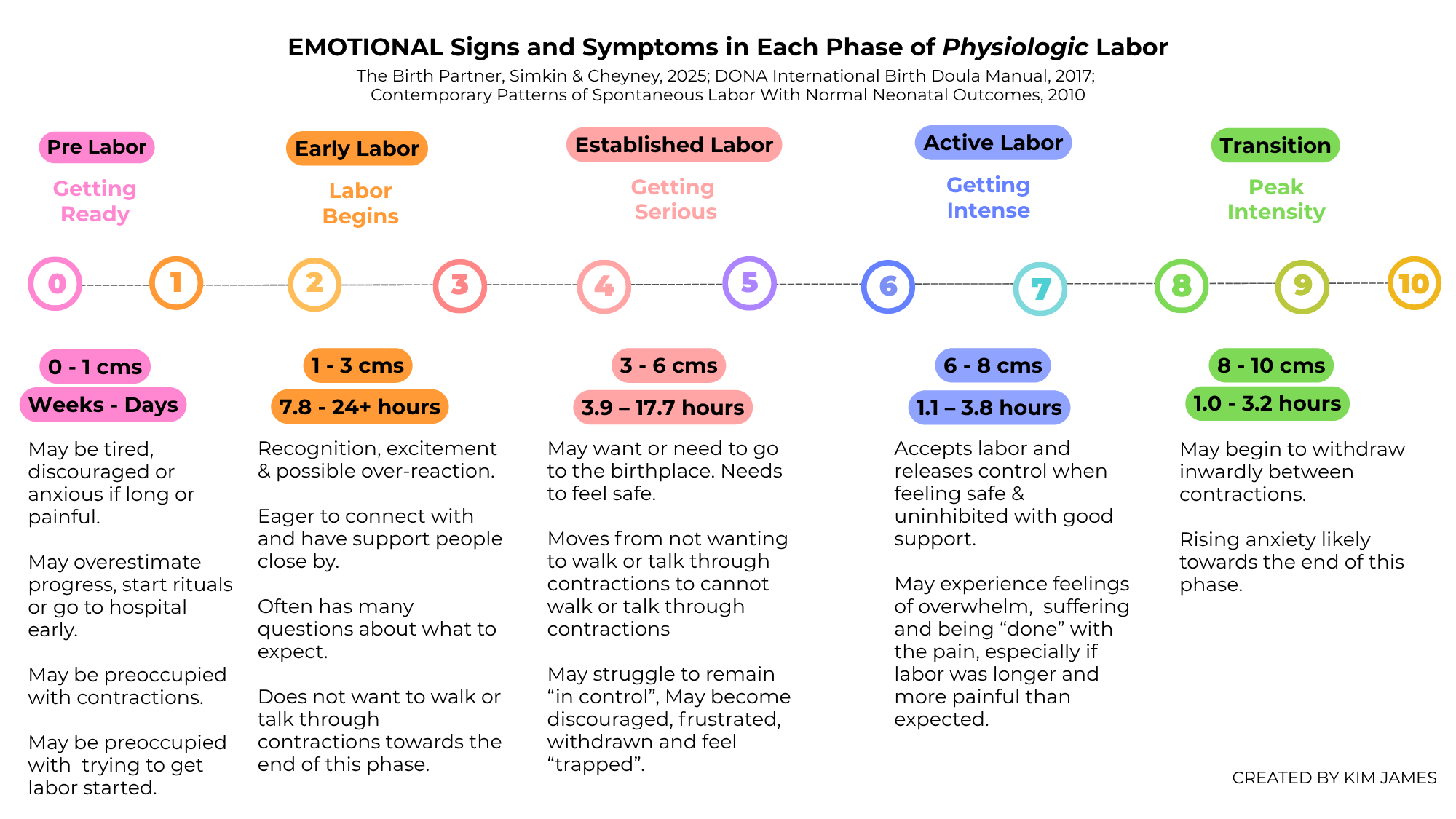
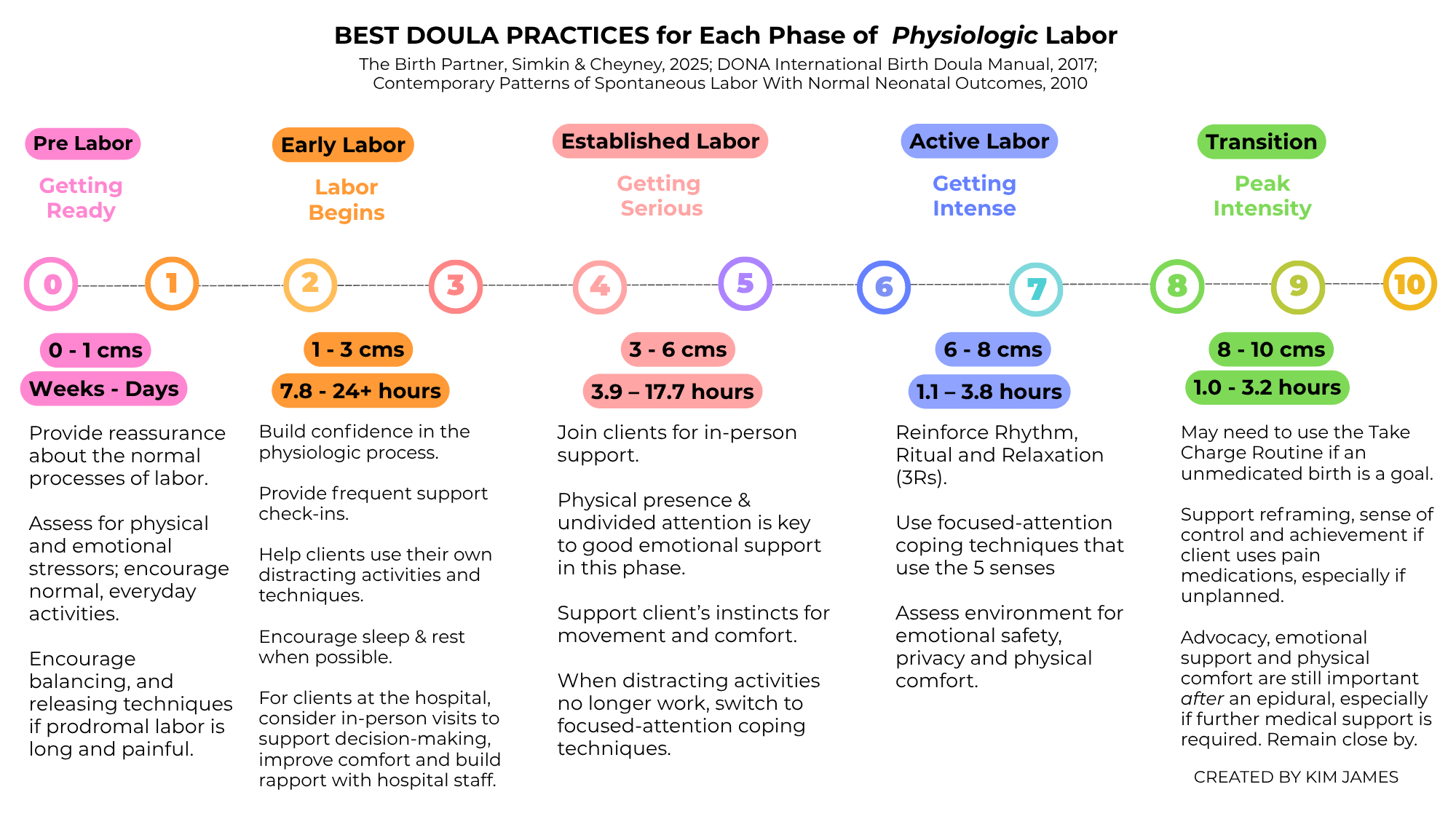
The solution may be to call out and rename the physiologic phases defined by their unique physical, emotional and psychological experiences by the birthing person, not just the acceleration of cervical dilation.
Here is how we might define and name the physiological phases of the first stage of labor to distinguish them and prevent confusion from medically active labor: Early labor, Established labor and Accelerating labor/Active labor.
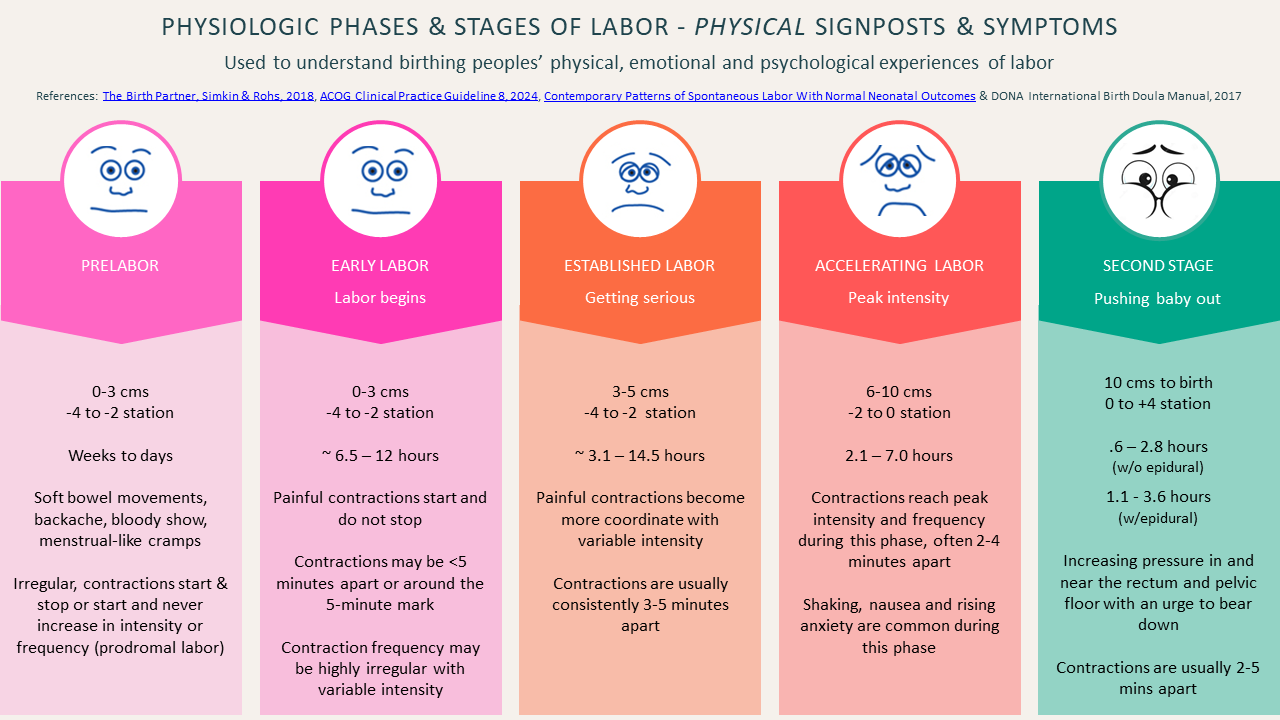
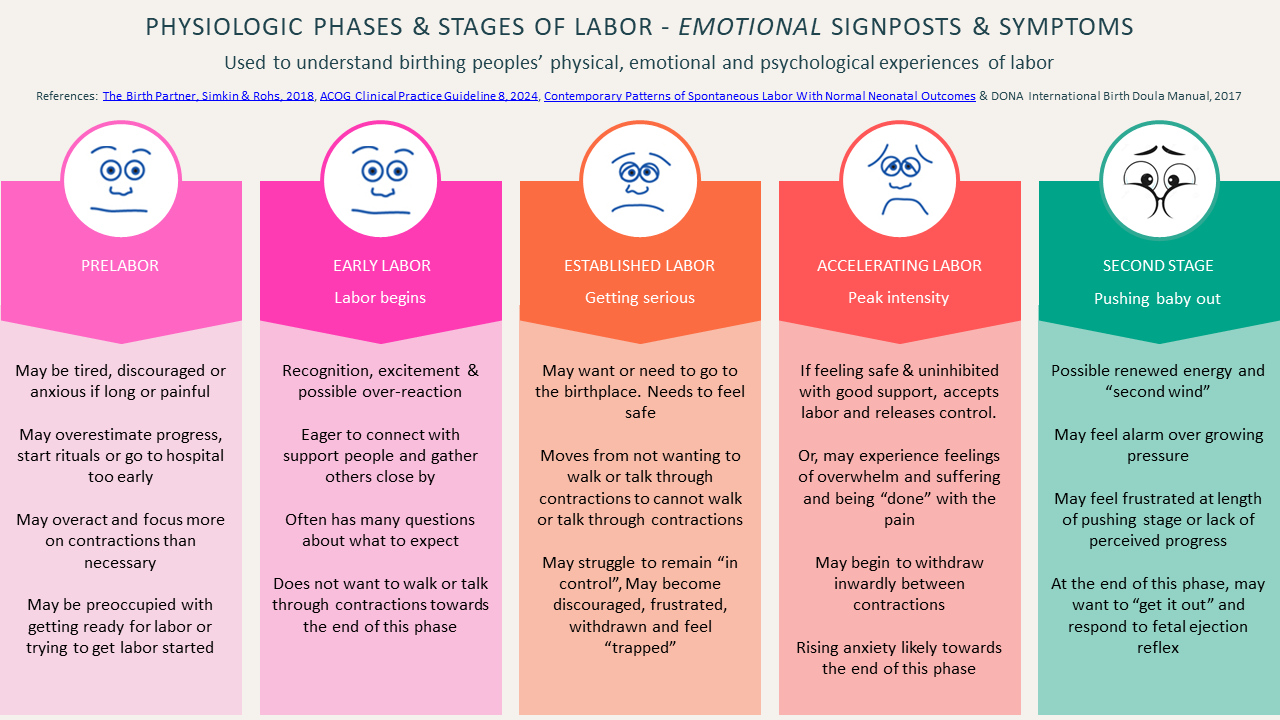
The doula uses the physiologic perspective to provide support in each unique phase so that the client feels their comfort, concern and care, whether remotely or in person.
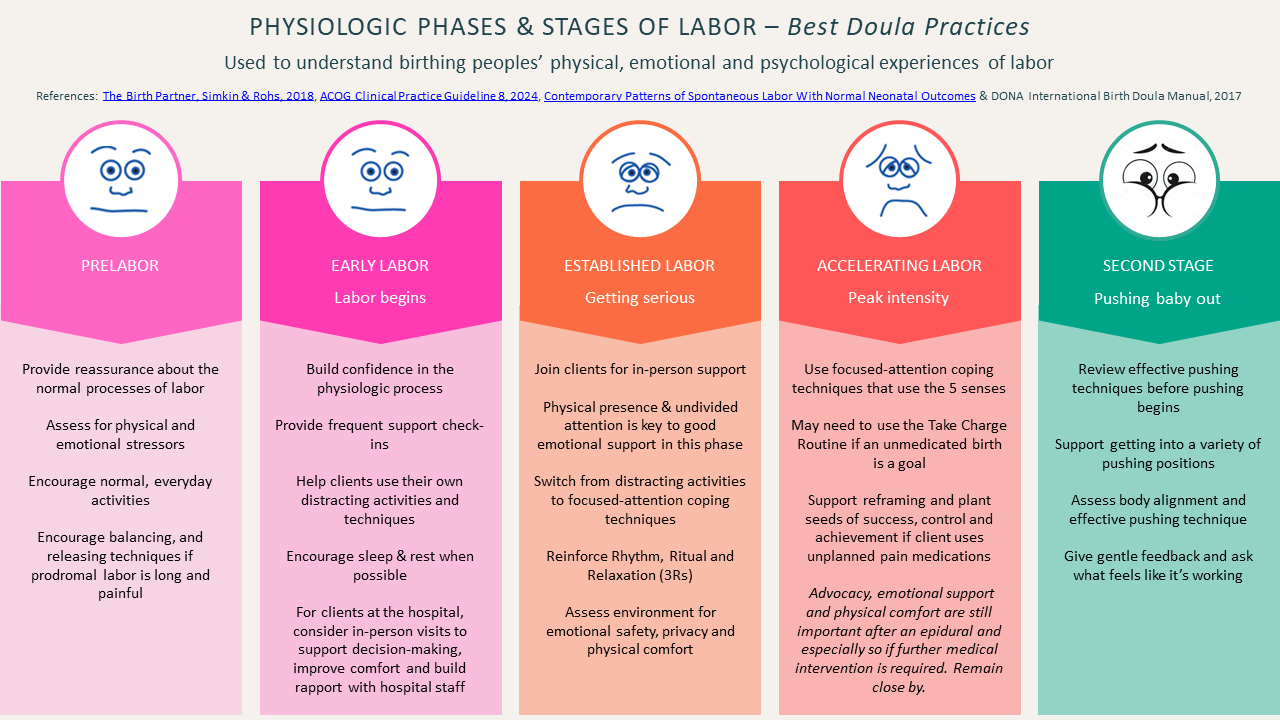
From these graphics, it’s clear the appropriate time for doulas to join clients for in-person support most often occurs during the early and established labor phases. In the average labor, 70% of the labor will be over by the time the acclerating (active) labor phase has begun, as has the opportunity to support many medical decisions, initiate advocacy and bolster clients’ confidence. Delaying or minimizing the need for in-person support until the accelerating, or medical “active labor” phase can be devistating for clients.
I urge doulas to carefully examine the language they use with clients to convey when and how we provide support. Let’s please consider abandoning the term active labor, leaving it for our medical care givers. Instead, let’s consider using terms and language that reflect the actual physical, emotional and psychological experiences of our clients.
We may also want to consider careful navigation of how we’re supporting the earliest phases of labor. To cement the trusting, nurturing relationships we’ve built prenatally, I urge doulas to practice the fine art of the early labor support ’pop-in’ that may be necessary for some clients, especially during long inductions. For more information on special support during inductions, please see our blog post on Gracefully Supporting Early Labor & Avoiding the Pitfalls of Under-Supporting Our Clients' Emotional Well-Being from 2022.
Promoting our clients’ emotional well-being and preventing trauma is parmount and primary to the doula’s role. A simple change of language and a good understanding of the physiologic phases of labor will help ensure we’re doing all we can to enhance our clients' mental and emotional experiences of their babies’ arrivals.
Byline
Kim James, BDT(DONA), ICCE, LCCE, CLE, NA-C
Owner & Operator of DoulaMatch.net
Certified Doula Swedish Medical Centers
Adjunct Instructor Simkin Center for Allied Birth Vocations at Bastyr University
Birth & Parenting Educator Parent Trust for Washington Children
References
The Birth Partner, Simkin & Rohs, 2018
ACOG Clinical Practice Guideline 8, 2024
Contemporary Patterns of Spontaneous Labor With Normal Neonatal Outcomes
DONA International Birth Doula Manual, 2017
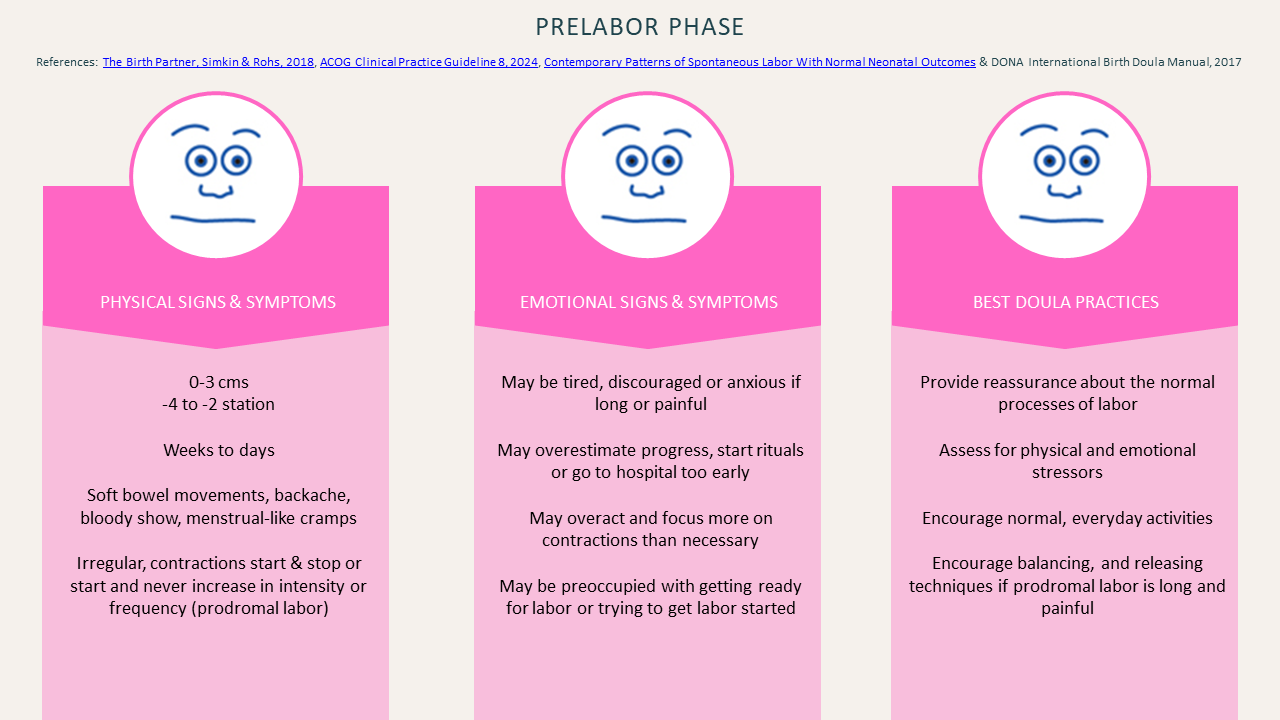
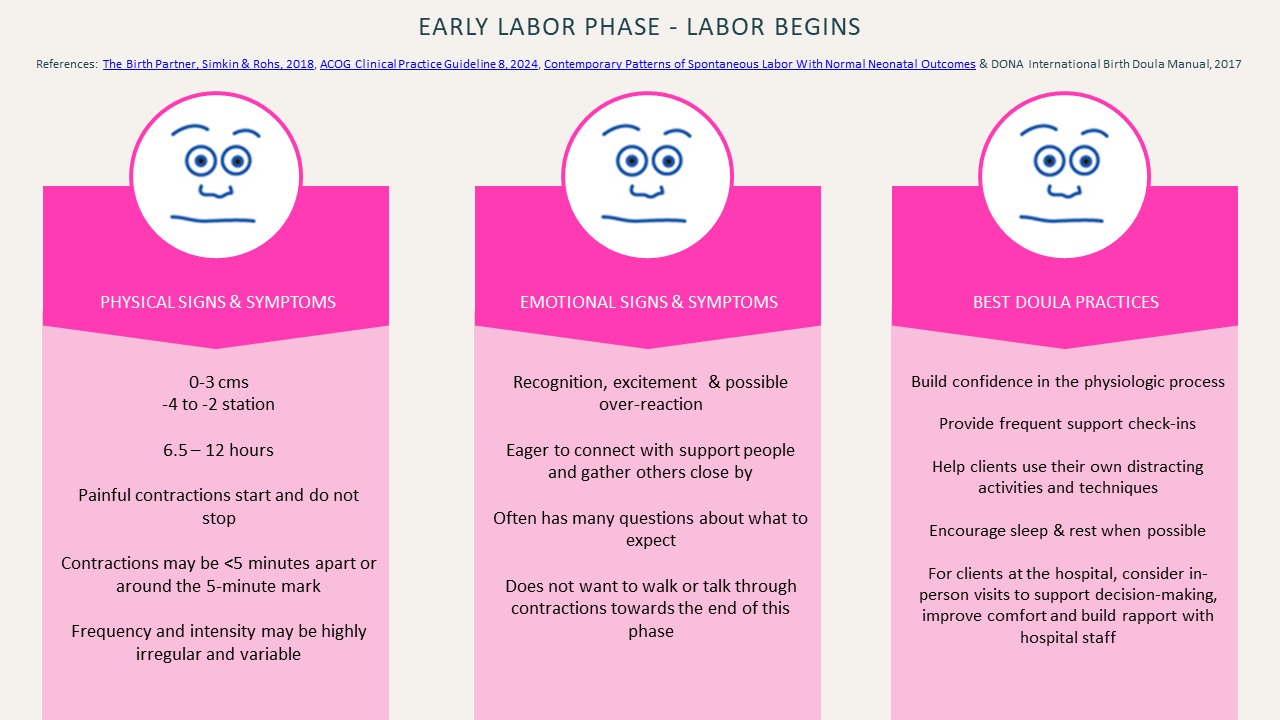
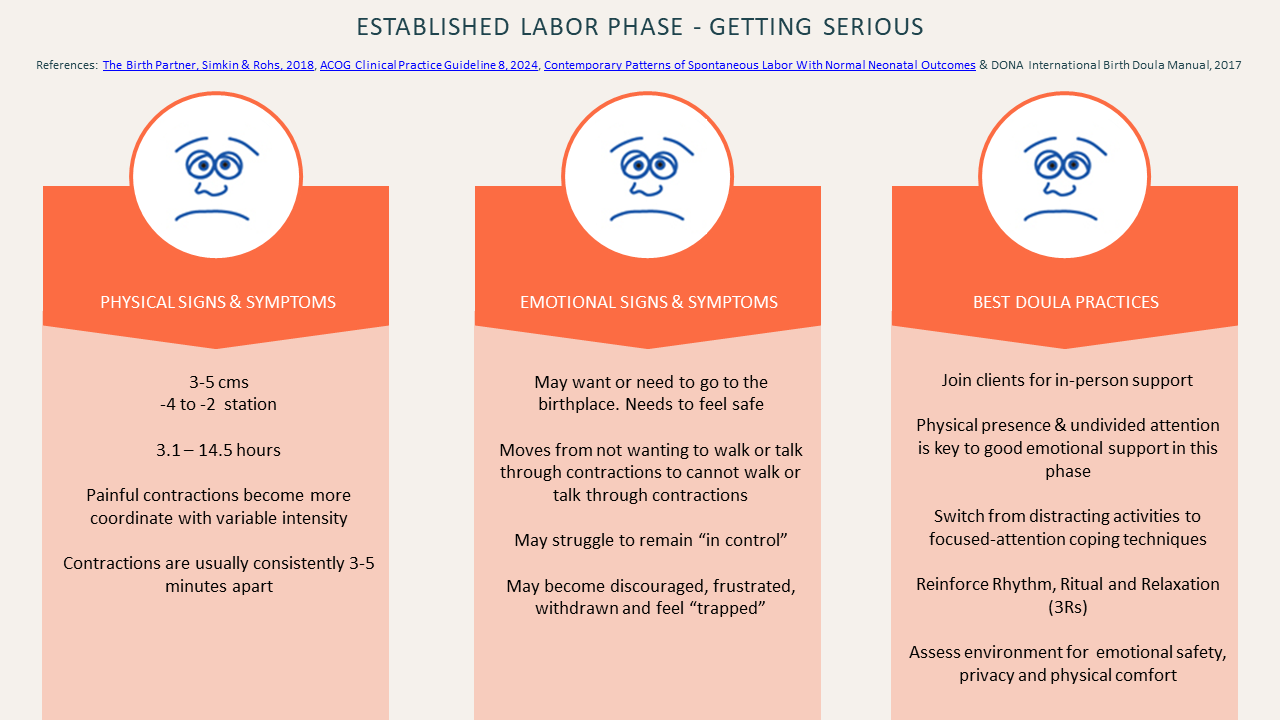
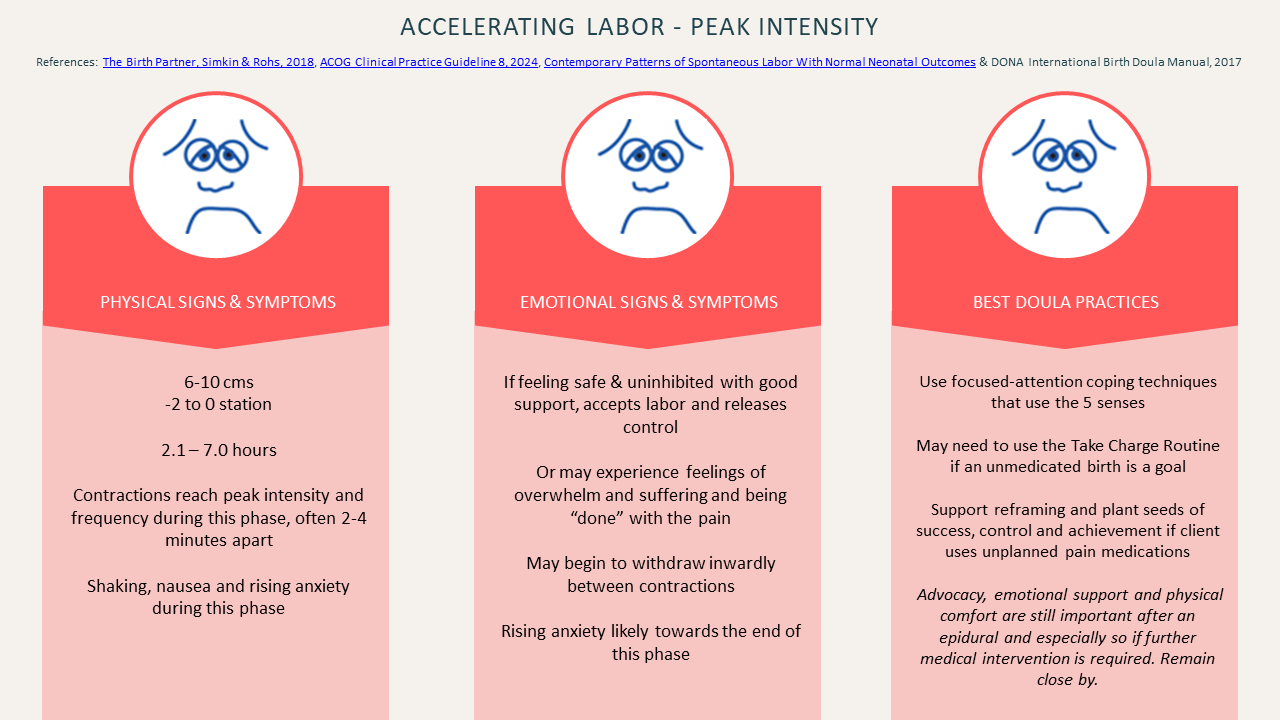
Additional graphics of the physiological phases and stages of labor:
Prelabor Phase
Early Labor
Established Labor
Accelerating Labor
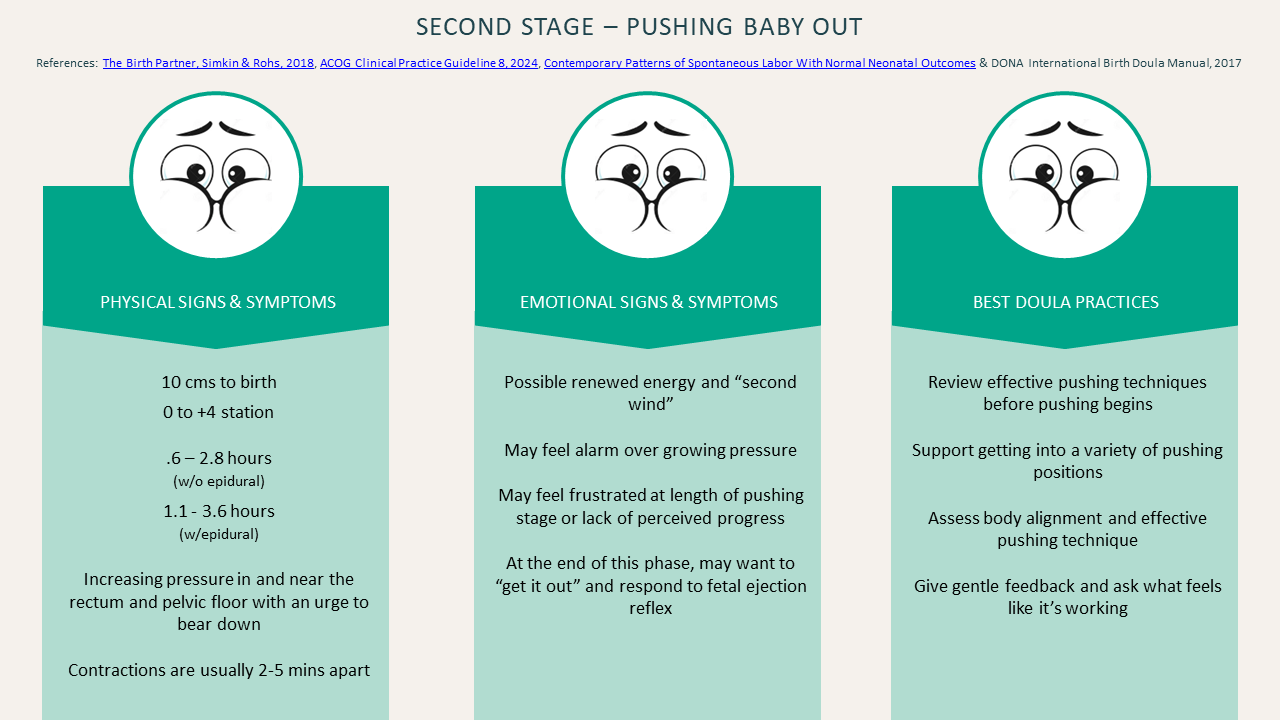
Second Stage